

Bartholin's abcess
This is an inflammation of a gland which is located in the wall of the vagina on either side. When an abscess forms this gland becomes filled with pus. When a cyst exists the fluid is not pus but a collection of fluid. A cyst which becomes infected leads to an abcess.
How did I get it?
A Bartholin's cyst or abscess occurs when the duct of the gland becomes blocked. The secretions are not able to flow out and build up. This often leads to infection.
Is It a dangerous condition?
It is not a dangerous condition but it may be very painful especially when infection occurs.
What will surgery do?
Surgery will release the fluid in the swollen gland and relieve the pain. If pus exists a patch of skin and cyst wall are removed and the whole cavity laid open. A pack is placed in the cavity and removed the following day. Thereafter healing occurs slowly until the whole area is obliterated. If the swelling is a cyst, this may be removed completely.
Can it come back again?
If done properly, it should not recur on the same side. However, there are two such glands; it is certainly possible for the process to occur on the other side in the future.
Is surgery for this condition dangerous?
The surgery itself is not dangerous, but as with any proceedure performed under general anaesthetic (where you are put to sleep), there is some minimum anaesthetic risk. Provided that you are in good health, this risk is small.
What about after the operation?
You will be instructed to sit in a solution of warm, salt water and dilute savlon (or some other mild antiseptic) for 15 minutes daily. This will relieve the soreness and pain. Alternatively, a half-hour soak in the sea is even better.
Can I work after the operation?
You will be allowed time to recover, which may be as long as 3 weeks. After you are completely healed you will be allowed back to work. Sea baths (or salt water baths at home) are often recommended for comfort and to aid the process of healing.
Can I function again normally?
Yes. After some initial soreness, the pain and swelling will disappear and normal sexual function can be resumed, usually in about 3 to 4 weeks.

Labour
(this is a long article)
While labour is a normal process, if you are about to undergo your first delivery there is bound to be some anxiety and concern, even fear. This is entirely natural. We have prepared this booklet for your information. If afer reading it carefully you still have concerns, please don't hesitate to call and speak to your doctor.
What is labour?
You have come to the end of your pregnancy and are preparing for the birth of your child. For the past several months (usually about nine) your unborn child has been nourished in the womb, snug and safe. The time has now come for him or her to leave the womb and breathe air for the first time. This is the moment you have been waiting for, partly with anticipation, partly with fear.
Labour is a complex process which culminates in the expulsion of the baby from the uterus. For the baby itself it is a traumatic event, for the uterus literally squeezes and pushes the baby through the birth canal. The uterus can do this because it is a very strong muscular sac, well equipped for its task.
The miracle is that until birth, the uterus is mainly quiescent, slowly growing in size to accommodate the growing child. At labour, this silence suddenly stops and the uterus begins the urgent process of ridding itself of its burden, its job finally done.
You have booked into the hospital where you plan to deliver. Your bags are packed with the necessary things you need for you and baby and stored in a place where you can easily reach them. Your doctor will be seeing you every week until delivery.
The waiting begins.................
How will I know when I am in labour?
Labour usually begins sometimes after the 36th week of your pregnancy. Most patients will deliver after the 38th week. A few may deliver at term and still some my go up to 2 weeks after their delivery date. These are all normal.
Labour begins with mild irregular contractions called tightenings. These may not be painful at first, but they gradually become more frequent and painful. When the contractions are occurring every three to five minutes and lasting for about 30 seconds or more you are in established labour. You need to alert the hospital and your doctor and go straight in for admission. Remember to take with you your notes from your doctor as well as your packed bag.
Are there any other signs I should be aware of?
Yes there are.
You may pass a mucous plug. This plug normally sits within the cervical canal. As the cervix dilates to make way for the baby=s head, the plug drops out of the canal. This heralds the onset of labour.
Your waters may break. You may feel a gush of fluid as the bag of water infront of the baby's head ruptures to make way for baby to descend. This may occur with or without pain. When this occurs you need to go to hospital immediately.
Any bleeding at this time, whether accompanied by pain or not should alert you to seek hospital admission immediately.
Be wary of an urge to stool. This is quite often the only signal some women have that they are about to deliver.
Be very conscious of the movements of your baby. Too much movement may mean that baby is distressed for some reason. Baby usually will sleep for some part of the day; during that time there will be little or no movement. If, however, you do not feel movement for a prolonged time, it could mean that something may be very wrong with your baby. In such instances, you need to contact your doctor or the hospital IMMEDIATELY.

How long will I be in labour?
If there are no complications, most women deliver within 6 - 8 hours of the onset of established labour. You will have a midwife in attendance while you are in labour. She will monitor your contractions to make sure that they are adequate. Your blood pressure as well as your urine will be tested at intervals and she will make sure that you empty the bladder every 2 hours. Your baby will also be monitored by the attending midwife. She will alert your obstetrician to any change in your baby's well-being.
Your doctor will also monitor your progress by a vaginal examination and if necessary your fore-waters will be ruptured to make way for baby. When you cervix is fully dilated, you are ready to deliver. At this time you will be transferred to the delivery room for your birth. Your doctor will be in attendance.
What sort of complications may prolong my labor?
Labour may fail to progress satisfactorily because
The baby’s head may be too big to come through the birth canal.
Your passage may be too small to allow baby to come though.
The baby's head though normal may not be sitting in the right position.
The contractions may not be of adequate strength and length to allow good progress in labour.
There may be maternal distress; these are medical conditions which make you tired, fatigued and unable to cooperate fully, such as hypertension, uncontrolled diabetes, etc.
There may be foetal distress; this is caused by factors which have a negative impact on the baby resulting in the heart rate either accelerating or decelerating with the contractions.
Unecessary heavy bleeding for whatever cause.
What are the possible results of these complications?
If any complications occur, your doctor will discuss them with you and your partner. Generally the onset of any complication will make it desirable to get the baby delivered as soon as possible to avoid further harm either to you or to the baby. Your doctor may follow one of several paths:
If your contractions are not adequate, then a drug can be used to strengthen them. This is given by drip into your veins.
If there is no progress because the fit is too small or if there is any sign that baby is in trouble, normal labour will be interrupted and caesarian section performed. Caesarian section is performed if in the doctor's opinion the safety of the baby and/or the mother is at risk.
What will my outcome be?
If there is satisfactory progress in labour, denoted by...
good contractions every 3 minutes
dilatation of the cervix to allow baby's head to come through
good descent of baby's head through the birth canal
and none of the complications mentioned above...
...your outcome will be full dilatation and normal delivery. If this is your first delivery, you may require an episiotomy to allow baby to come through the final portion of the birth canal. An episiotomy is an incision (cut) made under local anaesthesia in the lower birth canal and vagina.
How long will I remain in hospital after delivery?
You will be sent home about the second day. Lying in is essential for bonding with your baby and learning how to bathe and breast feed baby. This is also the time to learn how to do your vulval toilet especially if you have had an episiotomy sutured.
When can I return to work?
Maternity leave covers twelve (12) weeks; six weeks before and six weeks after the birth of your child. During that time you must remember to get as much rest as possible. Eating healthy meals is important since you will be breast feeding. Remember also to continue your iron supplements. Gentle exercise can be started immediately, like walking and swimming.
Daily sea baths are especially helpful if you have an episiotomy. In time you should resume more strenous exercises to help your abdominal and pelvic muscles regain their normal tone. Before you engage in heavy exercise like jogging or sports, be sure to get your doctor's permission. If you do start vigorous sporting activities remember to wear firm bra support to avoid painful movement of the breasts.

...But I'm so scared...
This is very natural, especially if this is your first child, or if you have had bad deliveries before. The truth is that the vast majority of deliveries are completely normal; chances are therefore that yours will also be normal.
If you have had previous problems, then your obstetrician will have alerted you to any anticipated difficulties with this current pregnancy and labour, and will have taken the necessary steps to lessen the impact of any foreseeable problems. You should make absolutely sure you follow any instructions given. "Cheating" is not only unwise, but could harm you and the baby. By cheating, I mean deliberately failing to observe recommendations and warnings. For example, many persons with swelling of the feet, high blood pressure or excessive weight gain may be told to rest in bed, or reduce their salt intake, or stick to a diet. Often some pretend to follow, but secretly cheat. This is really very unwise.
Finally,
..Your pregnancy and labour will be much smoother if you have enjoyed the full emotional support of your husband or partner.
There is absolutely no substitute for the love and concern that a truly committed partner can supply during this trying time. Make sure you involve him at all stages, if he is willing. Most centres are only too willing to allow your partner into the labour and delivery rooms, unless serious problems are foreseen.
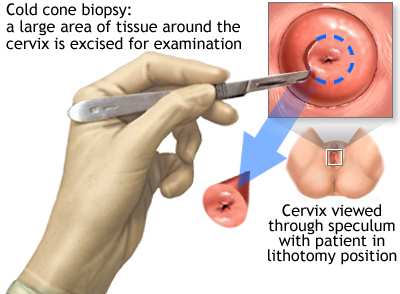
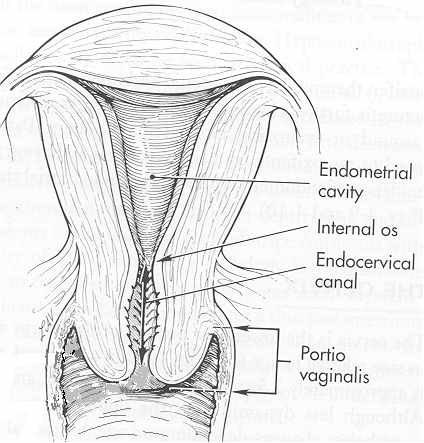
Cone biopsy
A cone biopsy is the procedure in which a cone-shaped portion of tissue is taken from the cervix. This is done in the operating theatre, usually under general anaesthesia.
Why do I need it?
A series of events have placed you in the category of women needing a cone biopsy. Your pap smear was abnormal and you had colposcopy done. You had a biopsy which showed that there was an abnormality of your cervix which needed removing for further study, specifically to see if there is any suggestion of cancer or pre-cancerous conditions. A cone biopsy was recommended.
Is this a dangerous condition?
In a sense it is, because if it is left alone and not treated there is a chance that it may become cancerous. The present condition in itself is NOT CANCER.
What will surgery do?
A core of tissue from the cervix will be removed including the abnormal area. This will be sent to the laboratory for a detailed examination.
Can it come back again?
Provided that the procedure succeeds in removing the complete area this is highly unlikely. However, a cone biopsy does not remove the entire cervix, which can of course develop other problems in the future.
Is surgery for this condition dangerous?
Usually not. Provided that you are in good health there should be no major problems. One complication which may be sometimes troublesome is bleeding. Great care will be taken to prevent this happening.
What about after the operation?
For a period of six weeks after the operation you should avoid lifting any heavy objects, wearing tampons during the menstrual period, and having intercourse. This is to ensure that unnecessary bleeding does not occur and that complete healing of the cervix takes place.
Can I work after the operation?
Work, especially heavy manual labour should be delayed till complete healing occurs. This is normally within 4 - 6 weeks after surgery, but light office or sedentary work can usually be resumed much sooner.
What about the future?
It is important that you continue having your pap smears on a regular basis. The first one after cone biopsy will be in 4 months, then every 4 months for the first year and yearly after that, if everything returns to normal.
Cryosurgery of the cervix means destruction of cervical tissue by freezing. This freezing is done by applying a cold metal tip to the cervix. This causes the tissue to become so cold that it dies.
Why do I need it?
You have had a biopsy of your cervix, the results of which show that there are abnormal cells or tissue on your cervix. These have to be destroyed and that is why you need cryosurgery.
Is it a dangerous condition?
The condition for which you are having cryosurgery is not usually serious. However, leaving it untreated for a long time may lead to more serious conditions developing, inccluing cancer.
What will cryosurgery do?
The abnormal surface area is rapidly destroyed by freezing. This is done by a special instrument called a cryo-gun, which uses nitrous oxide, a gas, to produce very cold temperatures.
Can it come back again?
Activity in your cervix is an ongoing process, so it can recur. The important thing is, however, to pick up the process early and prevent it from progressing any further by early treatment.
Is surgery for this condition dangerous?
This surgery is very minor, and is done in the office. You may experience discomfort in your lower abdomen while this is being done, or you may have hot flushing. These feelings will disappear after a short rest.
What about after the operation?
To avoid disturbing the healing process, for the first two (2) weeks do not use tampons, and please refrain from sexual intercourse for the same time. You may notice some spotting; this is normal. If you have an IUCD (loop) in the womb at the time of treatment, it will not be removed.
Can I work after the operation?
You can return to work immediately after this treatment. You will experience a rather heavy watery discharge shortly afterwards. This will continue for approximately 2 - 3 weeks. It would be a good idea for you to wear a panty liner for that time.
Can I function normally again?
Yes you can, as long as you follow the above instructions. It is extremely important that you keep your followup appointment since we will need to know if your treatment has been successful.
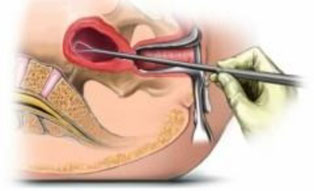
What is a D and C?
D and C stands for Dilatation and Curettage. The opening of the cervix is enlarged (dilatation ) and the cavity of the womb is scraped (curettage).
Why do I need it?
This is done usually as a means of arriving at a diagnosis for the following problems (among others):-
- Excessive or abnormal bleeding during or between the periods.
- Bleeding occuring after menopause.
- Heavy bleeding persisting after a miscarriage.
- In cases of infertility, to determine whether the ovaries are producing eggs normally.
Are these dangerous conditions?
They may be. The aim of a D&C is to find the precise cause for the problem so that a definitive treatment can be given, especially when abnormal bleeding occurs.
What will the surgery do?
The cervix (opening of the womb) is dilated and the inside lining of the womb is scraped away. New lining will then regrow replacing the malfunctioning one. The lining which is removed is sent to the laboratory for microscopic examination.
Can the problem come back again?
A D&C will normally stop any current abnormal bleeding. However, if other problems occur it is quite possible for bleeding to develop again in the future.
Is this kind of surgery dangerous?
A D&C is essentially a very simple operation with little intrinsic danger. It is usually done under a general anaesthesia for your comfort. You should be aware that any general anaesthetic carries some small risk. Provided that you are healthy, this risk is small.
In situations where the uterus is diseased, a D&C can indeed lead to complications such as a perforation. You will be alerted to any special considerations in your case.
What about after the operation?
You will not need to be kept in hospital, but will be sent home on the same day as soon as you have recovered from the anaesthetic. You may feel a bit tired and listless, a common feeling after an anaesthetic. It will wear off in a day or so. There may be some slight bleeding, but this too should stop after a few days. If it doesn't, you should alert your doctor.
Can I work after the operation?
In the usual case, you will need between two days to a week to recover sufficiently for normal work. You will be given medical leave for the appropriate period.
Can I function normally again?
Certainly. In time you will be perfectly normal again.

What is a normal delivery?
A normal delivery is one which proceeds naturally with minimal interference from doctors. It starts with the onset of labour and in most cases ends in the vaginal delivery of a healthy child. The vast majority of deliveries are normal.
Will mine be normal?
Provided that your pregnancy has been problem free, that you have no underlying complications (such as diabetes, high blood pressure, anemia etc), and that your obstetrician assesses the size of your birth canal to be adequate, you stand an excellent chance of having a normal delivery.
Can delivery be dangerous?
Problems can occur in any delivery, but remember that the vast majority of all deliveries are perfectly normal.
If you have had problems with past pregnancies, or have underlying medical disorders , these can affect the outcome of the delivery. Even if you have never had a problem, it is still possible to encounter unexpected difficulties.
How long will it last?
Labour without complications should take approximately 4 to 6 hours. It may be shorter, especially in the woman who has had many children before, but can also be much longer.
How do I know when I am in labour?
Labour begins with contractions of the uterus. It is these contractions which will eventually expel the baby from the womb. You are in established labour when you are having at least 4 contractions every 10 minutes. Be aware that an urge to stool may actually signal the onset of delivery.
Is it painful?
Yes it is, but you will usually be given just enough drugs to lessen the pain and help you relax between contractions. In this way labour progresses smoothly, with the minimum of discomfort to you and danger to the baby.
How will I know when I am ready to deliver?
You will usually feel an urge to strain or bear down. In some cases you may interpret this as a need to go to the toilet. When you feel this, it is wise to let the midwife know, as it generally signals that the time is near.
The midwife who attends to you will let you know when you are ready to be transferred to the labour room. An episiotomy (a small relaxing incision in the birth passage) may be done to assist you with delivery. This will be sutured afterwards.
Can I work after the delivery?
You will be given 6 weeks after delivery before you are required to return to work.
Can I function normally again?
Yes you will. However your body will take some time to recuperate from pregnancy and breast feeding. This is why it is advised that you space pregnancies adequately. You should also pay attention to post-natal instructions and exercises. These help your body return to normal strength as quickly as possible.
There is of course much more to be said about pregnancy and delivery. If you have any other questions or concerns, please feel free to ask your doctor. In addition, there are several online sites with excellent information about pregnancy.
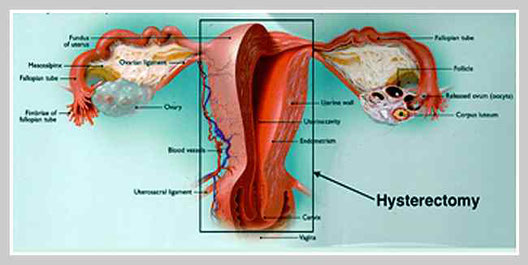
Hysterectomy
This is the removal of the uterus. Commonly the tubes and either one or both ovaries may be removed at the same time. This can be done via an incision across the lower abdomen (or more rarely in the lower midline of the abdomen). However it is now becoming the norm to have this procedure done laparoscopically via tiny incisions which heal with almost no visible scars.
Why do I need it?
This is done usually if you have fibroids which are causing problems, such as heavy menstrual bleeding, or protracted pain in lower abdomen. It may also be performed if fibroids suddenly start to grow quickly. Certain worrisome changes in the Pap smear results may also be a reason for having a hysterectomy.
Are these dangerous conditions?
They may be, since you may bleed so heavily that you may suffer from anaemia (low haemoglobin).
What will surgery do?
Surgery will remove the uterus, cervix, the tubes and one or both ovaries.
If bleeding or pain was the cause for your having the operation, this will usually be cured. Hysterectomies are done under a general anaesthetic where you are put to sleep, or less commonly a spinal, where you remain awake, but not aware of pain.
Can the problem come back again?
NO. Since there is no uterus, there will be no periods and hence no bleeding. If the surgery was done for a bad Pap smear, this problem will also have been corrected, since the cervix will no longer be present. You should know however that when this is done for pain, immediate or complete cure may not occur.
Is surgery for this condition dangerous?
It is important to remember that all surgery carries some risk and that complications can occur without warning. The main worry is bleeding at operation. Therefore surgery is done with due care and attention so as to minimize the amount of blood lost. Before operation a haemoglobin and a blood group are done to make sure that you are fit for surgery. The anaesthetist will also examine you prior to surgery.
What about after the operation?
Recuperation in hospital takes approximately three days. Thereafter you are given six weeks to recuperate at home. You may feel listless and tired during the initial stages, but a good healthy diet, rest and gentle exercise will aid in fast recovery.
Can I work after the operation?
Not before six weeks. At about 6 weeks you will feel well enough to return to work.
Can I function normally again?
You will function normally after. There is nothing that you did prior to surgery that you will not be able to do afterwards. Sometimes there are fears that one's sexual life will not be the same afterwards. In the majority of cases, such fears are groundless. However if you do have such concerns make sure you discuss them with your doctor thoroughly. If you think that your partner has worries about your sex life afterwards, you should also feel free to have the matter dicussed. Obviously you can no longer have children or a period after this operation.
What about the future?
You may exhibit post menopausal symptoms, like hot flushing, irritability etc, after the operation only if both ovaries are removed. In the event that both are removed, replacement therapy is started immediately after surgery. This will minimize the post menopausal symptoms. Your need for replacement therapy will be reassessed periodically.

What is an EPISIOTOMY?
This is a small cut made in the birth canal during delivery to assist in the delivery of your baby. It is done to avoid undue stretching and tearing of the vagina during delivery. A tear can sometimes be so bad that it extends into the rectum, causing severe problems afterwards.
Why would I need one?
An episiotomy is done to aid with the delivery of the baby's head. It helps the birth canal to allow the head to pass without undue stretching or tearing of the mother's tissues.
Is it a dangerous procedure?
Not at all, provided that it is done properly. Improperly done, it can however cause severe problems, as when a cut is made inadvertently into the rectum. To avoid this happening, an episiotomy is usually made from the vagina to one side, rather than directly downwards. This avoids damaging the rectum.
How is an episiotomy done?
During the delivery a small cut is made in the birth canal between the vagina and the rectum, under local anaesthesia. Great care is taken to avoid damaging the rectum or anus.
What will happen to the area after?
After baby is born and the afterbirth is removed, the area is sutured to close the defect.
Will there be pain after?
There will be no pain at first, but as the anaesthetic wears off, there will be some discomfort. You will get some tablets to alleviate the pain.
What about after the operation?
You will be asked to have sea or Sitz baths. Sitz baths are a combination of warm salt water in a small amount of Savlon solution. You will sit in it for about 30 minutes three times a day. This will lessen the discomfort considerably.
Can I work after the operation?
Within a week of having an episiotomy you will feel better, but you will not return to work for 6 weeks after delivery.
Can I function normally again?
When the area has finally healed, it will be as before. In the early stages however, you may have some discomfort when you begin intercourse after delivery. That will get better with time. In any event, you should allow at least three to six weeks before attempting intercourse. If in doubt, contact your doctor.

What is foetal monitoring?
This is a relatively simple but important examination done in the office. Using an electronic device called a foetal monitor, a number of important characteristics of your baby are assessed. These include the heart rate, the frequency with which the baby moves around in the womb, and how the baby's heart responds to movement and other stimuli.
Why do I need it?
Sadly many women carry a pregnancy to term (or very nearly there), only to lose the child days or weeks before the expected delivery date. This is often due to problems that are present in the womb, but are undetected often until it is too late. One of these is an umbilical cord that has a knot in it, or is wrapped around the child's neck. In either of these conditions, a fatal outcome can occur during pregnancy when the flow of blood is suddenly cut off before the baby is fully born.<br>
Foetal monitoring can often pick up these dangerous but silent situations by noting how the baby's heart responds to it's own movements.
Is foetal monitoring dangerous to the baby?
As far as is presently known, not in the slightest. The instrument uses ultrasonic waves to detect the baby's heart beats. There are no Xrays or other harmful radiation. You will be shown how to signal the instrument when you feel any movements, and for about 30 minutes a continuous record is made of baby's heart rate, movement and (in some cases) uterine contractions.
What if the test is abnormal?
There are different kinds of abnormality that can be seen on the resulting tracing. Generally a baby that does not move, or a heart rate that slows down markedly on movement indicate the possibility of trouble during a later vaginal delivery. Clearly every case will not be the same. Your doctor will discuss your individual tracing with you. However, a very worrisome tracing may indicate the need for a Caesarean section in order to gaurantee the baby's safety.
At what stage in my pregnancy will monitoring be done?
This is done in the last trimester, usually after the 32nd week. In some situations it may be necessary to repeat the test if an initial result revealed a problem.
Is the procedure painful for me?
Not at all, since it does not involve any needles, injections, or internal examinations. You will be put in a comfortable reclining position, and given a small push-button. All you will be required to do is to push the button whenever you feel the baby move. The foetal monitor itself will do the rest using external probes applied to the abdomen.
How long does the test last?
About 30 minutes usually. This may be extended if special problems arise.
Can I work again after this procedure?
Usually, yes. Please understand though, that if a serious abnormality is suspected on the basis of the test, your doctor may advise you to go into hospital immediately.
Special comments.
Be reassured that the vast majority of all pregnancies and deliveries are completely normal. But for the woman who loses a child, this is a disaster.
Foetal monitoring is an attempt to predict the isolated cases that, while appearing to be normal, may nevertheless run into serious trouble during late pregnancy or delivery.

What is induced labour?
This is the act of artificially starting the process of labour, usually by drugs given intravenously (into the veins). These drugs act on the uterus and stimulate it to contract.
Why do I need it?
This procedure is contemplated when you are at term and delivery is delayed for some reason. It may also be required if there is some complication in your pregnancy which may cause more harm to baby in the womb than if it were delivered. It may also be necessary if you suffer from high blood pressure in pregnancy, if you are a diabetic or if you are carrying twins.
Are these dangerous conditions?
Not usually. But they may lead to the baby becoming distressed. When this happens the baby's heart rate slows. If this slowing is significant it is wise to deliver baby sooner rather than later. Anything that causes distress of the baby can lead to fetal harm, even death.
What will happen to me when I am induced?
You are prepared for delivery with a shave and an enema. A drip is placed in your forearm and a drug given to bring on contractions. When you are in labour, the waters are 'broken'. If the pains become distressing to you, an injection is given to help ease the pain; this also causes you to relax.
How long will it last?
You are allowed at least 6 hours in labour. You are monitored by the nurse to make sure that both you and baby are fine. When you are ready for delivery you will feel like bearing down or wanting to pass stool. You will be taken into the delivery room and prepared for the final stage of delivery.
What are the possible results of induction of labour?
One of two things may occur; either your progress is satisfactory and you deliver normally, or there is little or no progress. In the latter case a Caesarian Section may become necessary.
How do I know what my outcome will be ?
Satisfactory progress is signalled by :-
- good contractions every 3 minutes.
- the cervix opening to allow baby's head to come through.
- baby's head descending through the birth canal.
An internal examination is done every 4 - 6 hours to determine progress of labour.
Can I work after the procedure?
You are given six weeks to recuperate after delivery, after which you can return to work.
Can I function normally again?
Most women like to wait until after the postnatal check to resume sexual activity. Provided you have not been specifically cautioned about resuming activity, it is usually quite safe once the post-delivery bleeding has ceased. If you are in doubt, please contact your doctor.

What is a LAPAROSCOPY?
This is the term applied to a surgical procedure in which the contents of the abdomen are inspected through a special telescope, which is introduced into the abdomen through a tiny opening made usually just under the navel.
Can I function normally again afterwards?
Certainly. After full recovery you will be back to normal.
Why do I need it?
Laparoscopy is a diagnostic procedure and is used in a vast number of medical situations. One of the most common is pain in the lower abdomen, in which case it is used to help determine the cause of the pain. Knowing the exact cause of the pain is vital for accurate treatment. It is also widely used in the investigation of infertility. Laparoscopy is also being used for a growing number of surgical procedures. One such very common operation is tubal ligation (tie off).
How is the procedure done?
Through a small cut under your navel the laparoscope is introduced into your abdomen, after you have been put to sleep. This allows your organs to be seen as well as any abnormalities that may be present. If a biopsy needs to be done or if your tubes need to be tied, these can also be done.
Is this sort of surgery dangerous?
Not usually. The operation is well tolerated by any healthy person. Complications are minor and the vast majority of women having this surgery leave hospital the same day. However it is well to remember that any procedure done under a general anaesthetic always carries some risk.
What about after the operation?
The surgery is done on an outpatient basis. This means that as soon as you recover from the anaesthetic (an hour or so), you will be allowed home. Mild discomfort in the abdomen is normal, and passes quickly. Unless you have been advised otherwise by your doctor, you may eat, bathe etc normally.
Can I work after the operation?
Since you will have a general anaesthetic (where you are put to sleep), you will need a few days to rest and recover. More time may be given at the discretion of your doctor if more extensive surgery has been done.

What is a MYOMECTOMY?
This is the removal of fibroids from the womb or uterus. The womb is left in place so that future child-bearing is not compromised. Fibroids are benign tumours that commonly form in the muscular wall of the uterus. They often cause no symptoms but occasionally can be the reason for heavy menstrual bleeding (which can then lead to anemia), abdominal pain and an unsightly, large abdomen. Very rarely, fibroids become malignant (cancerous).
Why do I need it?
You have been diagnosed as having fibroids which have been causing one of the following problems:-
- Heavy and/or painful periods.
- Persistent pain in the lower abdomen.
Your fibroids have been discovered to be growing rapidly.
This method of treating fibroids is reserved for women who want to have children in the future, or do not want the uterus removed for whatever reason.
Is it a dangerous condition?
Fibroids are very common, and many women are not even aware of their presence. However fibroids can cause you to bleed so much that you become anaemic; that is your haemoglobin can drop to the point where you experience tiredness and fatigue. If it drops too low, you might need a blood transfusion.
What will surgery do?
Under a general anaesthetic (where you are put to sleep) the fibroids in the uterus will be removed. The common method of doing this involves an incision (cut) in the abdomen through which the uterus can be accessed. However these long incisions are painful and waiting for them to heal results in long absences from work. Increasingly this kind of surgery is being done laparoscopically, through tiny incisions in the abdomen which heal quickly and with little discomfort. Often the person can then resume productive work in a week or so.
Can they come back again?
Yes they can. But fibroids usually grow slowly so that you may need treatment only once.
Is surgery for this condition dangerous?
Any major operation does carry some risk. Provided that you are healthy, this risk is small. It will increase somewhat if you suffer from other medical conditions like diabetes, >high blood pressure, etc. One other risk in this operation is that of major bleeding. The uterus is well supplied with blood vessels, and sometimes bleeds uncontrollably during an attempted myomectomy. If this occurs, it may become necessary to remove the entire uterus. Happily, this event is rare.
What about after the operation?
You will have some pain in your abdomen after the operation, but you will be given pain killers to alleviate this.
Can I work after the operation?
You will need about 6 weeks to recuperate after surgery if you had a long incision. If surgery is done laparoscopically, you should require less than a week. Thereafter you will be able to resume work.
Can I function normally again?
Yes you will. You are completely normal after recovery. A good precaution is to wait for about 12 to 18 months after surgery before trying to become pregnant.
Special Note:
This surgery can now be done laparoscopically - that is, instead of a relatively long incision in the abdomen, the uterus can now be removed via tiny incisions using a procedure called with special instuments, including fibre-optic cameras, which permit viewing and operating on organs without widely opening the abdomen. The result is shorter post-operative convalescence and less pain. You can also resume work much sooner.
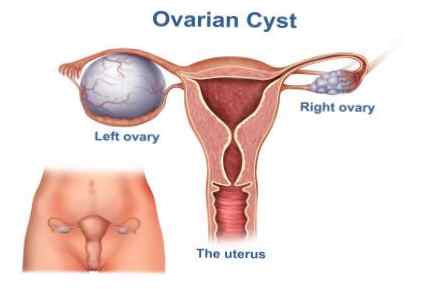
What is an ovarian CYSTECTOMY?
The ovaries are two slightly oblong organs in the pelvis on either side of the womb. An ovarian cyst is a swelling on the ovary consisting of fluid in a cavity. Ovarian cystectomy is the term given to the operation to remove such a swelling.
Why do I need it?
During a physical, or as a result of having had an ultrasound examination, you have been diagnosed as having a cyst on the ovary. The ovaries frequently have small cysts as part of their normal status, but this cyst is much larger than normal. Your doctor has recommended removal of the cyst to determine its nature.
Is it a dangerous condition?
Most swellings of the ovaries are benign (not cancer), and are therefore not at all serious. A few, however, may turn out to be cancer, which is always a serious disease.
What will surgery do?
To be sure of the nature of the cyst it is necessary to obtain some (or all) of the tissue for the pathologist to study. At surgery, the swelling on the ovary, with or without a portion of the ovary itself, is removed. The other ovary may also be biopsied to make sure that there are no swellings in it.
Can it come back again?
This depends on the nature of the swelling. If your ovary has the tendency to produce simple cysts, then they can recur. If the swelling is benign, but is such that the entire ovary is removed, no recurrence will occur, since the ovary has been removed. If the swelling is discovered to be a cancer, you will be kept under surveillance for the rest of your life to detect any signs of recurrence. Further therapy may also be indicated.
Is surgery for this condition dangerous?
As with all major surgery, there is always some risk. If you are healthy, and the swelling is small and benign, the risk is minimal. Diabetes, high blood pressure, obesity, extreme old age, or other medical problems increase the risk, as does a very large malignant tumour.
What about after the operation?
You will have an incision (cut) in the lower abdomen, which usually heals speedily. Most of your pain and discomfort will rapidly improve, and you should quickly be back to normal. If both ovaries have had to be removed, you may experience hot flushing and other unpleasant sensations. Your doctor should be contacted for advice.
Can I work after the operation?
Not immediately. You are given four to six weeks in which to recuperate after which you should feel well enough to return to work.
Can I function normally again?
Yes, you can. This will not inhibit you in any way. Normal sexual activity can be resumed as soon as you feel up to it. Your reproductive function will be as good as it was before unless both ovaries have been removed.
Special Note:
Most surgeries on the ovaries can now be carried out using a procedure called laparoscopy. This utilizes pencil thin instruments, including special fibre-optic cameras which permit visualization of, and operations on, abdominal and pelvic organs without making a long cut in the abdomen. The result is less post-operative pain and a shorter time to recovery.

What is normal pregnancy?
You have discovered that you are pregnant. This was diagnosed by the fact that you missed your period or a pregnancy test confirmed that you are pregnant. This leaflet contains a few guidelines to make your pregnancy as smooth as possible.
What do I do now?
You should see your obstetrician, who will see you every month until you are approximately 32 weeks. Thereafter you will be seen two-weekly until 36 weeks and then weekly until delivery.
Are there any dangers?
As you already know, pregnancy is a normal event which will not usually pose a serious threat to your safety provided that you are basically healthy. But any pregnancy can develop difficulties. It is the task of your doctor to monitor you carefully throughout your pregnancy to make sure that all goes well, or to intervene if a problem manifests itself.
How will I be monitored?
This takes place in several stages. At your first visit an ultrasound and blood test will be ordered. The ultrasound will date your baby and will also make sure that it is normal and healthy. The blood test will note your blood group and your haemoglobin. The haemoglobin will be repeated once a month, to make sure that baby is getting enough iron for growth. A repeat ultrasound is done at 32 weeks, at which time you may request to be told baby's sex, if you so desire.
How can I look after myself during pregnancy?
You should continue to have a good healthy diet. Continue to do whatever you normally do, including exercise in moderation. This is healthy. If however, there are any complications, you will be told when you should stop any risky activity. To ensure that neither your nor your baby's health suffers, you will be given iron and vitamin suppliments commencing at 16 weeks. It is imperative that unhealthy practices like smoking and excessive alcohol drinking BE STOPPED during pregnancy. A positive outlook and good emotional support are indispensable during this time.
How do I know when I am ready for delivery?
You will be seen every week for the last four weeks of pregnancy. Your pelvic passage will be assessed to see if baby can be born naturally. Contractions will begin, erratically, then become more constant. You should monitor these. When they become regular every five minutes, you should prepare yourself for hospitalization. You should then call your doctor who will make arrangements for you to be admitted at once.
What can I expect at delivery?
You will feel the urge to bear down when you are ready to deliver. You will be transported to the delivery room and prepared for delivery. It is important that you listen to the instructions given by your attending nurse and doctor. With every contraction you get during delivery, you must bear down or "push in your bottom" to facilitate the birth of your baby. Failure to do this may retard the delivery and result in a Caesarian section. The placenta is delivered after your baby is born. You will be given an injection to prevent hemorrhage. You will be allowed to cuddle your baby as soon as it is born. If you do have an episiotomy or tear, this will be sutured immediately after the area has been deadened by local anaesthetic.
Can I have my husband or partner with me?
Your husband or boyfriend can attend at your delivery. He is more than welcome, provided he is not the fainting type! We've had spouses fall flat on the floor during deliveries and really don't want this to happen!.
After delivery, what?
You will be able to leave hospital on the third day after delivery. Your baby will be seen by the pediatrician of your choice. You will be reassessed 6 weeks after delivery.
NB Both antenatal and postnatal classes are held at Bayview Hospital. Antenatal classes start from 32 weeks onwards. If you want to attend, and this is recommended, kindly let us know, so that arrangements can be made.
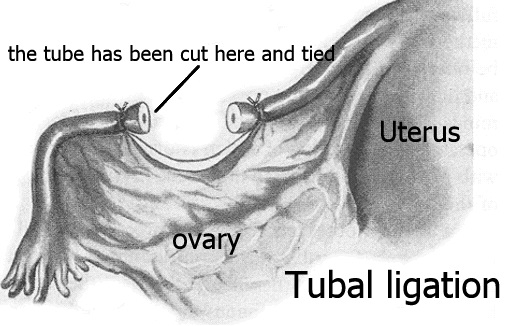
What is a tubal ligation?
A tubal ligation is the operation designed to tie off the Fallopian tubes. These lie in the pelvis on either side of the womb just above the ovaries, and must be open in order for normal pregnancy to occur. Tubal ligation therefore is an operation designed to make further pregnancies impossible. It is a sterilization procedure performed in the female. The analogy in the male is vasectomy.
Why do I need it?
A tubal ligation causes permanent sterilization, so preventing you from having any more children. Though in theory it can be reversed in case you change your mind later, you should be aware that it is designed to be permanent. If you want to have children in the future, DO NOT opt for this method, unless you discuss your plans with your doctor.
What will surgery do?
At surgery, both tubes are identified and either tied or burned and then cut. In cases where you may want to have them untied later, a special clamp may be applied to the tubes. This can be removed later.
Can the tubes be untied afterwards?
In the majority of cases the answer is no except where only a small portion of tube is removed. In that case, it may be possible to rejoin the cut ends back together. If the special clamp was used, then it is possible to remove it later. However, you should be warned that your ability to become pregnant may be permanently reduced, and that "untieing" the tubes provides no guarantee of pregnancy.
Is surgery for this condition dangerous?
No, provided that you are fit and healthy. Other medical conditions like diabetes, high blood pressure or extreme obesity all tend to increase the risk.
What about after the operation?
You will have some mild post operative discomfort, which can be alleviated by simple pain killers.
Can I work after the operation?
You will always be given time to recuperate after surgery. By the time you have recovered you will be able to work normally.
Can I function normally again?
Yes you can. Having a tubal ligation in no way permanently disturbs any bodily functions, and has absolutely no adverse effect on your sexual ability or enjoyment.
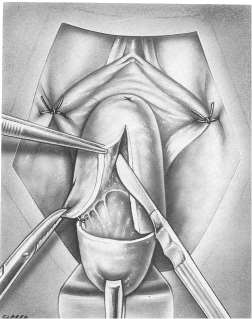
What is a vaginal hysterectomy?
This is the term used when a hysterectomy is performed through the vagina instead of through a cut on the abdomen. This is usually done when the muscles and ligaments supporting the uterus are weak. This results in the uterus and bladder "falling" into the vagina. In some cases it may "fall" right through the vagina and appear as a lump which can be seen projecting from the vagina. This is called a prolapse.
How did I get this condition?
It is widely thought that persons who suffer from this condition have a congenital weakness of the supporting tissues of the pelvis. In addtion repeated child birth makes the floor of the pelvis weak especially if the babies were big at birth. Prolapse normally occurs in the older age group , usually after menopause.
Is it a dangerous condition?
With the weakness of the muscles, the uterus, bladder and rectum can drop. This may lead to the distressing problem of stress incontinence, where a few drops of urine involuntarily escape from the bladder every time you laugh, cough or strain. In addition, the prolaspsed organs can become infected. However, the condition is not usually dangerous.
What will surgery do?
Surgery will remove the uterus through the vagina. The muscles and ligaments will all be repaired and placed back in their normal positions. At the same time, the weakened muscles are strengthened and tightened to provide better support.
Can it come back again?
Normally it does not.
Is surgery for this condition dangerous?
Any surgery done under a general anaesthetic has some inherent risk. Provided that you are fit and healthy this risk is small. Diabetes, high blood pressure, extreme old age or other medical conditions will add to the normally small risk. You will be checked and investigated before the operation to make sure that this risk is kept as small as possible.
What about after the operation?
You will be given six weeks to recuperate after surgery. It is important to move around and remain active even though there will be some initial discomfort.
Can I work after the operation?
Once recuperation is complete you can return to work.
Can I function normally again?
Yes, you can. Many women as well as their partners often harbour major fears about a hysterectomy. There is absolutely no reason why you should suffer any lessening of your sexual ability or enjoyment after surgery. However, if problems arise in this area, feel free to discuss it with your doctor.

What is vaginitis?
An irritation or inflammation of the vagina, producing an abnormal discharge, generally accomapnied by itching and soreness of the vagina and external genitalia.
Is vaginitis serious?
No. Vaginitis is not generally very serious. It is estimated that one out of every two women will have vaginitis at least once. Most will suffer nothing worse than a temporary annoyance.
What causes vaginitis?
Fungi, bacteria or other microscopic parasites. Chemicals in commercial douches and vaginal sprays can sometimes cause a "non-infectious" vaginitis - which is why many physicians discourage their use.
How do you "catch" vaginitis?
Some women may be infected by their sexual partners. (Men rarely have symptoms, but may carry the infective organisms.) In other cases, bacteria from the feces may get into the vagina because of careless wiping after a bowel movement.
However, many cases of vaginal infection are not "caught" in the regular sense of the word. There are always lots of tiny microbes or "germs" living in our bodies. Normally they do not cause any problem. On occasion however, they may invade the vaginal tissues and cause infection, esp when the normal resistance of the vagina is altered, as can happen in pregnancy, or when you are taking antibiotics.
What is the most common form of vaginitis?
Moniliasis caused by a fungus, is probably the most common form of vaginitis at this time. It is also known as candidiasis (or yeast infection). The main symptom is a thick white discharge that produces marked genital itching.
How is moniliasis treated?
By a variety of medications: vaginal tablets, suppositories, creams, solutions, ointments, or oral tablets.
What are the other types of vaginitis?
Trichomoniasis, caused by a microscopic parasite, produces an odorous, yellowish-green discharge with itching. Nonspecific vaginitis results from an overgrowth of normal bacteria in the vagina. Viral vaginitis is caused by a virus related to the organism that causes herpes. An ointment or lotion will relieve the discomfort.
Atrophic vaginitis occurs in women whose ovarian function has ceased either because of age or surgery. Absence of normal hormones makes the vaginal walls unusually thin. Gonorrhoea and other sexually transmitted diseases are the most serious causes.
Can I have more than one vaginal infection at a time?
Yes. Mixed infections are quite common and, like all forms of vaginitis, should be seen by your doctor.
What will happen when I see my doctor?
After a cerful history to determine whether you are taking any medication, or if you are preganant, you will be examined, and a sample of your discharge taken for diagnosis. That's why it's important not to douche before your appointment.
How will my doctor diagnose the condition?
In many cases simple inpection of the discharge provides a clue. Laboratory testing of a sample of the discharge (a swab) will furnish proof of the cause.
Can I stop the itching myself?
Don't experiment. Check with your doctor.
How long must I take my medication?
You may feel better within a few days, even a few hours. But though your symptoms have vanished, the organisms that infected you will probably still be active. Play it safe. Follow your doctor's instructions to the letter.
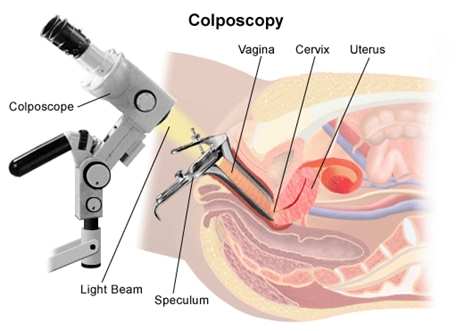
What is colposcopy?
This test entails looking at your cervix through a special instrument which magnifies the cervix and so enables the doctor to see very small abnormal areas clearly.
Why do I need it?
Either your recent Pap smear was abnormal or you have had a series of abnormal Pap smears. These indicate that there is some sort of unusual process affecting the cervix. By viewing this area under magnification areas of unusual activity can often be seen and biopsied (sent to the lab for assessment).
Is this dangerous?
Not necessarily. It alerts one to the fact that some abnormal activity is occurring in your cervix. Since this activity is abnormal it should not be left alone as it may lead to something more serious, possibly cancer.
What will be done at colposcopy?
A vaginal speculum (an instrument which allows one to clearly see the cervix and vaginal walls) will be placed in the vagina. The cervix is treated with a special solution which will highlight any abnormal areas. A special stain may also be used to highlight these areas. This will be discussed with you at the time of the examination. If a biopsy needs to be done, you may feel mild discomfort, but severe pain is usually uncommon.
What will happen after?
This will depend of course on what is found at colposcopy. If treatment is required this will commence just after your next period. You will be given a appointment for this.
Will I need any treatment?
Not necessarily. In many cases, though, some form of treatment will be needed. This may include various vaginal creams or a LOOP CONE BIOPSY. You will get some information about this treatment before you leave the office, or will be directed to our website where you can read the relevant information.
What about after the procedure?
The findings will be discussed with you, and steps taken to proceed to definitive treatment if needed. There will be no discomfort or bleeding after colposcopy, (since this is essentially a visual examination) unless a biopsy was also required.
Can I work after the operation?
Yes, of course.
Can I function normally again?
Yes. Having a colposcopy done in no way affects any of your normal bodily functions.